Evaluating Point-of-Care Ultrasound Systems & Clinical Use Case
When evaluating a new point-of-care ultrasound (POCUS) system, clinical leaders, educators, and hospital buyers may feel bombarded with top-tier lists, technical specification sheets, brand comparisons and more. However, as we explored in our recent guide on the Clinician-Centered POCUS Framework, choosing a system based purely on hardware specs is a flawed approach.
The reality is that rankings are often misleading because they ignore the environment in which the device will be used. The “best” point-of-care ultrasound depends entirely on what you are trying to do – and what tradeoffs matter most in that specific moment. For instance, no single handheld ultrasound device is best across all clinical scenarios; in a 2024 comparison of six handheld systems, POCUS experts rated image quality, ease of use, and portability as the most important attributes, and no device was superior across all views.1
To help decision-makers navigate this landscape intelligently, this evaluation guide breaks down POCUS systems by clinical use case. By examining what matters most clinically in different scenarios, we can better understand how different system designs address those unique needs.
Table of Contents
- Evaluating Point-of-Care Ultrasound Systems & Clinical Use Case
- Emergency Medicine and Trauma: The Need for Speed and Clarity
- Vascular Access: Precision and First-Pass Success
- Cardiology and Intensive Care: Diagnostic Depth and Quantification
- Primary Care and Outpatient Clinics: Screening and Scalability
- The Evolution of POCUS Design
- References
- Additional References
- Q&A: Evaluating POCUS Systems by Use Case
Emergency Medicine and Trauma: The Need for Speed and Clarity
In the emergency department or trauma bay, a clinician’s primary goal is rapid stabilization and triage. Point-of-care ultrasound systems serve as a dynamic, real-time tool to answer immediate, life-threatening questions. The clinical priority here is the speed of deployment and immediate image clarity. For instance, clinicians performing an Extended Focused Assessment with Sonography in Trauma (EFAST) exam need to quickly identify free fluid in the abdomen or chest, or pericardial fluid, typically within three to five minutes, with data clarifying that EFAST is specifically ideal for ruling-in traumatic injuries leading to faster diagnosis and treatment.2

However, evaluating systems for this environment involves distinct tradeoffs. Traditional, high-end cart systems offer excellent image quality but are notoriously bulky and difficult to maneuver into a crowded trauma bay. Conversely, ultra-cheap handhelds are highly mobile but may lack the processing power to provide high-confidence imaging when time is of the essence. The ideal system boots up quickly, is easy to disinfect, and avoids complex controls.
Dr. Josè Pinto, a general surgeon and POCUS advocate, emphasizes that advanced AI features – like automated anatomical labeling – are incredibly beneficial in these high-stress environments to confirm a clinician’s interpretation of on-screen anatomy in real-time.3
Vascular Access: Precision and First-Pass Success
Placing a peripheral intravenous (PIV) catheter is a fundamental healthcare skill, yet up to 30% of adults and 50% of children are estimated to have difficult venous access (DVA).4 Clinically, what matters most is high-resolution superficial imaging that allows clinicians to see target veins clearly, differentiate them from arteries, and track needle advancement in real time. The ultimate goal is to increase first-pass success rates, minimize patient discomfort, and avoid unnecessary escalation to expensive central venous catheters (CVCs). A 2018 meta-analysis found higher success with ultrasound-guided peripheral IV placement than with palpation/direct visualization (81% vs 70%), with fewer punctures and less time to access.5

When evaluating systems for vascular access, a high-frequency (5-15 MHz) linear array transducer is the absolute gold standard, with ASE guidance noting that high-frequency linear probes (about 8–12 MHz) provide superior spatial resolution for structures near the skin surface.6
While basic, wireless handheld units offer great mobility, some can suffer from image lag or signal drops during the procedure. On the other hand, cart-based systems provide premium resolution but are overkill for standard med/surg floors and are too cumbersome to easily integrate into bedside workflows. The most effective systems for vascular access strike a balance: they offer the portability of a tablet-based system but utilize a direct, wired probe connection to guarantee a stable, zero-lag signal for precise needle tracking.
Cardiology and Intensive Care: Diagnostic Depth and Quantification
Perhaps the biggest challenge in defining the “best” ultrasound is the human factor andIn critical care and cardiology settings, the clinical requirement moves far beyond a subjective “eyeball” estimation of the heart. Precision medicine demands objective, quantifiable data, such as a definitive Left Ventricular Ejection Fraction (LVEF), which is a fundamental measure of the heart’s pumping power and dictates therapeutic pathways. Clinicians also require advanced capabilities like Continuous Wave (CW), Pulsed Wave, and Tissue Doppler Imaging to assess complex hemodynamics and valvular conditions.
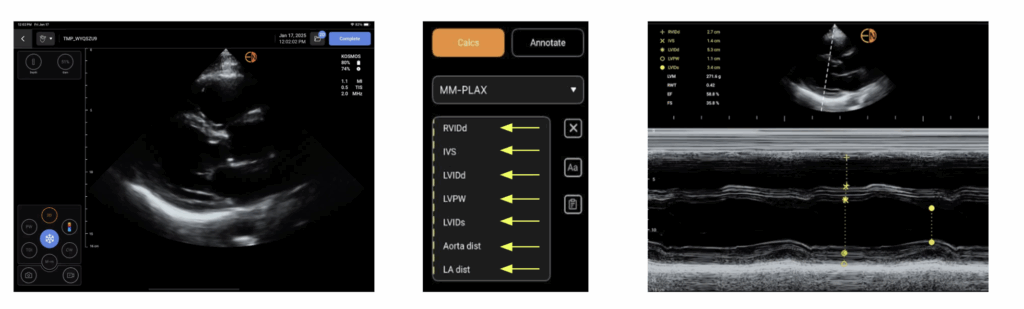
This use case highlights the starkest contrast in the POCUS market. Most affordable handheld probes lack CW Doppler entirely, rendering them insufficient for comprehensive cardiac exams and traditionally forcing hospitals to purchase high-end cart systems costing upwards of $50,000. To resolve this, a new tier of “High-Value Hybrid” systems now provide cart-level diagnostic power – such as gold-standard PZT crystal technology and diagnostic-quality CW Doppler – in a highly portable format.
Furthermore, a prospective multicenter study, elucidated that AI-assisted FoCUS LVEF assessment showed highly reproducible LVEF estimations that rival traditional echocardiograms.7 These AI algorithms can calculate the LVEF using the biplane Simpson’s method in less than 20 seconds, drastically outperforming the 2-3 minutes required for manual tracing on traditional carts.
Primary Care and Outpatient Clinics: Screening and Scalability
As healthcare shifts toward early intervention, primary care and outpatient clinics are increasingly utilizing POCUS to detect diseases before they require hospitalization. In these settings, scalability, low training burdens, and cost-effectiveness are paramount. The goal is to act as a diagnostic filter, ensuring that specialized tertiary care is reserved for those who truly need it. A 2019 systematic review in the Annals of Family Medicine noted that POCUS in general practice leads to improved and earlier diagnoses, though its success is highly user-dependent and requires appropriate training and quality assurance.8
The steep learning curve of traditional ultrasound often causes severe bottlenecks, while some modern handheld devices trap clinics in mandatory subscription models that diminish the long-term value of the investment. AI guidance is transforming this space by enabling rapid upskilling.
In Malaysia, the “Heart2Miss” initiative run by Dr. Diana Foo successfully utilized Kosmos portable, AI-powered ultrasound to train novices with no prior medical background in just four weeks.9 The AI provided real-time guidance on probe positioning, allowing these new users to effectively screen diabetic patients for heart failure, proving that modern POCUS can successfully offload the diagnostic burden from centralized hospitals. In the PANES-HF study, novices with no prior echo experience achieved interpretable AI-guided studies using Kosmos in 96 patients after 2 weeks’ training, with sensitivity 84.6% and specificity 91.4% for detecting LVEF <50%, though the mean scan time was 12 minutes 51 seconds.10
The Evolution of POCUS Design
When evaluating POCUS options, clinical leaders should step away from standard feature checklists. The best system is the one that directly addresses the workflow bottlenecks of your specific department.
We are currently seeing the emergence of highly adaptable platforms designed to resolve these traditional tradeoffs. Systems like Kosmos provide a prime example of this evolution. By offering cart-benchmarked diagnostic tools – including advanced Doppler and AI-driven capabilities – without the massive footprint of a cart or the subscription traps of basic handhelds, the platform provides clinicians with the consistency, guidance, and ease of use required to deliver superior patient care. Ultimately, intelligent evaluation means prioritizing the clinical objective first, and finding the technology that supports it.
References
- EchoNous. What Is the “Best” Point-of-Care Ultrasound? A Clinician-Centered Framework. EchoNous Blog. Published 2026. Accessed March 4, 2026. https://echonous.com/expert-consensus-best-point-of-care-ultrasound-framework/
- Netherton S, Milenkovic V, Taylor M, Davis PJ. Diagnostic accuracy of eFAST in the trauma patient: a systematic review and meta-analysis. Can J Emerg Med. 2019;21(6):727-738. doi:10.1017/cem.2019.381
- EchoNous. Dr. Josè Pinto: A Surgeon’s Perspective on the Evolution of POCUS and Trauma Assessment. EchoNous Blog. Accessed March 12, 2026.
- Bahl A, Johnson S, Alsbrooks K, Mares A, Gala S, Hoerauf K. Defining difficult intravenous access (DIVA): a systematic review. J Vasc Access. 2023;24(5):904-910. doi:10.1177/11297298211059648
- Mitchell EO, Jones P, Snelling PJ. Ultrasound for pediatric peripheral intravenous catheter insertion: a systematic review. Pediatrics. 2022;149(5):e2021055523. doi:10.1542/peds.2021-055523
- Vegas A, Wells B, Braum P, et al. Guidelines for performing ultrasound-guided vascular cannulation: recommendations of the American Society of Echocardiography. J Am Soc Echocardiogr. 2025;38(2):57-91. doi:10.1016/j.echo.2024.12.004
- Motazedian P, Marbach JA, Prosperi-Porta G, et al. Diagnostic accuracy of point-of-care ultrasound with artificial intelligence-assisted assessment of left ventricular ejection fraction. npj Digit Med. 2023;6:201. doi:10.1038/s41746-023-00946-9
- Andersen CA, Holden S, Vela J, Rathleff MS, Jensen MB. Point-of-Care Ultrasound in General Practice: A Systematic Review. Ann Fam Med. 2019;17(1):61-69. doi:10.1370/afm.2330
- Foo DHP. Decentralized community-based rapid cardiac ultrasound triage for early heart failure detection using a hub-and-spoke model: findings from Heart2Miss initiative. Paper presented at: European Society of Cardiology (ESC) Heart Failure 2025; May 18, 2025; Belgrade, Serbia.
- Huang W, Koh T, Tromp J, et al. Point-of-care AI-enhanced novice echocardiography for screening heart failure (PANES-HF). Sci Rep. 2024;14:13503. doi:10.1038/s41598-024-62467-4
Additional References
- Hernandez Torres SI, Ruiz AJ, Holland LA, Ortiz RF, Snider EJ. Evaluation of Deep Learning Model Architectures for Point-of-Care Ultrasound Diagnostics. Bioengineering. 2024;11(4):392. doi:10.3390/bioengineering11040392
- EchoNous. The EchoNous Guide to Ultrasound-Guided IV Access. EchoNous Blog.
- van Loon FHJ, Buise MP, Claassen JJF, Dierick-van Daele ATM, Bouwman ARA. Comparison of ultrasound guidance with palpation and direct visualisation for peripheral vein cannulation in adult patients: a systematic review and meta-analysis. Br J Anaesth. 2018;121(2):358-366. doi:10.1016/j.bja.2018.04.047
- EchoNous. Beyond a Good Squeeze: How to Get LVEF on Kosmos Three Ways. EchoNous Blog.
- Papadopoulou SL, Sachpekidis V, Kantartzi V, Styliadis I, Nihoyannopoulos P. Clinical validation of an artificial intelligence-assisted algorithm for automated quantification of left ventricular ejection fraction in real time by a novel handheld ultrasound device. Eur Heart J Digit Health. 2022;3(1):29-37. doi:10.1093/ehjdh/ztac001
- EchoNous. From Rural Reality to Revolutionary Research: The Inspiring Journey of Dr. Diana Foo. EchoNous Blog.
Q&A: Evaluating POCUS Systems by Use Case
A system overloaded with features you don’t use in your specific clinical environment represents a low-value investment. For example, paying a premium for a massive cart system in a fast-paced emergency department may hinder your workflow rather than help it, due to its lack of mobility and difficult disinfection process.
While handheld devices offer excellent portability and a low entry price, their diagnostic depth is frequently limited. Many lack essential cart-level features like Continuous-Wave (CW) Doppler or advanced AI measurements. Additionally, many popular handhelds require mandatory annual subscription fees just to keep the device functional, which drastically lowers their long-term value.
The evaluation should focus on high-frequency linear array imaging (5-15 MHz) and system reliability. Because precise needle tracking is required to navigate around valves and arteries, devices that offer a stable, zero-lag image – often via a direct wired connection to a tablet – are generally preferred over wireless units that may experience signal interference.
A High-Value Hybrid is a new category of ultrasound that bridges the gap between basic probes and expensive carts. These systems, led by the Kosmos ultrasound system from EchoNous, pack the advanced diagnostic features of a high-end machine (like full Doppler suites and advanced AI) into a portable, affordable package, typically offered as a single, one-time purchase without recurring software subscriptions.