Will Point-of-Care Ultrasound (POCUS) Become the Fifth Pillar of the Physical Exam?
A Conversation with José Mariz

Dr. José Mariz, MD, PhD
General Internist
EchoNous
Marketing Team
Dr. José Mariz, MD, PhD an esteemed general internist and educator deeply committed to advancing Point-of-Care Ultrasound (POCUS) recently spoke with the marketing team at EchoNous. In this discussion, we explore the transformative potential of POCUS and its role in shaping the future of medical practice.
[Note: This interview has been edited for clarity and brevity.]
Background and Journey into Ultrasound
EchoNous: Your journey into medicine and ultrasound is truly unique. Can you share what inspired your path, especially given your diverse background and experiences?
José Mariz, MD, PhD: I’m a general internist in a classical way, well-versed in various hospital areas. My eldest cousin, a doctor, influenced me. My family does not have a tradition of studies and we were from a rural background in Portugal.
My mindset is unique. I love making connections. Internal medicine is my sweet spot, where I feel at home. Too much rigidity stresses me, I thrive on change. I’m a doer, you know.
My ultrasound journey began 22 years ago, working in the ED alongside radiologists when the technology was still emerging. Over the past two decades, the radiology landscape has undergone significant changes. Despite initial skepticism about my internal medicine background, I proposed a fellowship in ultrasound to my department chief, inspired by a dedication to continuous learning.
As a university professor in 2005, we introduced ultrasound into anatomy lessons using a massive machine, collaborating with an anesthesiologist for catheter insertions. Being self-taught, I liken the process to using a knife rather than a light bulb, mentally piecing together and interpreting body sections for imaging.
Teaming up with Marco Antonio, a like minded physician from Brazil, we initiated an ultrasound program in Campinas during 2010. This involved hosting Brazilian colleagues for a week-long course and case validations. In 2013, formal teaching commenced, and I engaged in collaborative projects, such as the EchoNous venture and AI image classification.
Co-founding POCUSX, one of Portugal’s first POCUS education program, was truly my passion project. It’s this fantastic B-learning journey into point-of-care ultrasound, all about hands-on learning and personalized teaching. We’re like the pioneers here, breaking new ground in Portugal and offering our students the freedom and flexibility you don’t get from the usual universities. We’re big believers in the future of personalized education and ensuring our students have all the tools they need to thrive.
EchoNous: We love hearing about POCUS journeys—each one is unique, especially as ultrasound becomes part of the medical equation. Thanks to dedicated physicians like yourself and growing educational options, more individuals are embracing point-of-care ultrasound.
Learning ultrasound is a journey that takes time. When you started, it was more challenging than it is now with more true POCUS products available. It’s impressive that you were motivated enough to overcome that challenge and continue your education.
José Mariz, MD: In 2008, I had to use an old machine from GE from the 90s. It took 6-7 of us to put it in the van, driving about 25 kilometers, feeling a bit like hair-raising moments along the way, you know?
EchoNous: That machine probably weighed as much as the van!
José Mariz, MD: Yeah, I think so!
POCUS Education Challenges: Breaking Barriers

EchoNous: Times have changed, for sure. The challenges in POCUS education are something you’ve been actively addressing. What advice do you have for newcomers? Do you agree that education is a significant barrier?
José Mariz, MD: Absolutely. It’s the most significant barrier, and I think it’s because ultrasound is often confused with radiology and learning imaging, but it’s not. It’s totally different. It’s about clinical work happening at the bedside.
The turf wars between ultrasound and radiology are settling because radiologists understand the importance of the clinical majority at the bedside, at the point of care. The challenge with teaching point-of-care ultrasound in this way is that we have to teach clinical aspects of the physical exam and clinical reasoning and integrate that with the rest of medicine.
It’s more manageable for me as an internist, given my training in patient care. Others focus on specific applications, like anesthesiologists with central venous catheters and nerve infiltrations. Yet, the real challenge lies in integrating point-of-care ultrasound as the fifth pillar of the physical exam.
For the past 200 years, we’ve relied on the stethoscope, deeming it the pinnacle of physical exams. However, it’s an evolutionary journey [that is] altering our perspective on patient assessments. Ultrasound, much like developments before it, is revolutionizing the physical exam.
Only some people see it as I do, but some cardiologists use these terms. Even though cardiologists mainly deal with the heart, they connect the dots in the broader context of the patient’s narrative beyond just the heart exam. It’s not merely a technique; gynecologists use similar reasoning. Intriguingly, we are having many talks with radiologists about correlations in point-of-care ultrasound when gynecologists have been doing it for 50 years.
Imagine going to any country, rich or poor, and finding a pregnant woman without an ultrasound. That’s a bit odd. It should be the same for an internist. How could this be possible? An internist should take the lens when there’s an opportunity to see if there is any fusion. It’s interesting to see the resistance, even from colleagues in my specialty; that’s a big challenge.
EchoNous: Absolutely, ultrasound isn’t just limited to imaging. It’s there to guide your treatment of patients. It helps you understand the story of what’s happening so you can direct the care. It’s not a threat to radiology or cardiology professions; it’s helping you do your job better.
José Mariz, MD: Right. There is evidence that in the south of Spain, they implemented a POCUS program in the healthcare system which led to an increase in the number of ultrasound exams ordered. The relationship between primary care doctors and radiologists improved because they learned to ask more focused questions. This is crucial from a probabilistic standpoint, as performing exams with a clear clinical question may yield relevant findings. First, it is essential to consider why the exam is necessary.
I just returned from a meeting at the university where two colleagues and I discussed incorporating ultrasound into pre-graduate studies. The director of my university course is highly interested in point-of-care ultrasound and the outlook is very promising for all stakeholders. This is truly exciting because we haven’t witnessed a revolution in clinical practice like this since the inception of the status quo; it’s historical, you know, it’s history.
The Role of Artificial Intelligence in POCUS Education
EchoNous: Excellent insights. As an educator, what do you find most challenging for individuals using point-of-care ultrasound?
José Mariz, MD: The main challenge is creating a well-structured portfolio for autonomy, emphasizing hands-on experience over theoretical knowledge. An eight-hour immersive course and practical encounters with an expert focusing on motor skills are crucial. Artificial intelligence aids learning by narrowing focus and accelerating comprehension.
Incorporating ultrasound into regular practice is another obstacle, requiring about 25 cases per window and 320 cases in an ideal scenario. Managing this workload, discussing cases, and seeking human validation are significant challenges. While AI contributes, peer-to-peer discussions remain crucial for certification. Balancing technology and the human aspect is critical for a comprehensive and validated approach. The challenge lies in finding this balance, ensuring certification from a colleague in a peer-to-peer context. It’s challenging because you need human validation alongside AI to maintain a comprehensive approach.
Transforming Ultrasound Education
EchoNous: Thank you for sharing that perspective. Can you say more about POCUSX? What unique contributions did you aim to contribute to ultrasound education that weren’t there before?
José Mariz, MD: I’ve been conducting courses for a decade, over 150. Despite putting in a lot of effort, I found myself stuck in a routine that didn’t prioritize what truly mattered: constructing a portfolio and teaching the “why” behind ultrasound. That’s why we created POCUSX, which, as far as I know, is the first of its kind in Portugal – a formal academy offering courses. Unlike traditional courses held in hotels, where the physical gathering is a one-time event, POCUSX is different.
POCUSX ensures ongoing support and is readily available for ultrasound guidance. We collaborate regularly with ultrasound machines, complementing hospitals without aiming to replace them. Our structured and constant presence is similar to the Gulf Coast Ultrasound Institute in the United States.
EchoNous: You mentioned the importance of POCUS and the common barriers to its adoption, such as education and access to technology. While some companies focus on making ultrasound more accessible, they often neglect the crucial education aspect. POCUSX addresses this challenge by providing ongoing support to ensure users become proficient. Hospitals need help staffing physicians and training everyone, which can be a heavy load. POCUSX is doing a great job in this area.
José Mariz, MD: Hospitals face many problems. Like a big boat sailing in the ocean, it’s difficult for hospitals to train staff in real time while the ship is sailing. It’s dangerous and unrealistic. Cooperative efforts and strong education are vital.
I’m not trying to dismiss the value of the newer wave of individuals entering the field. It’s about acknowledging that I’ve invested 22 years of hard work, gaining valuable experience as both a practitioner and a teacher for 15 years. The real challenge in effective teaching arises when you’re continuously in the thick of it. To teach well, you’ve got to hit pause and reflect, and that is not even sometimes feasible in the fast-paced university setting. There are always some pieces that need to be added that are crucial for effective teaching.
AI: A Game-Changer in Point-of-Care Ultrasound
EchoNous: We didn’t start working on AI because it was trendy. We did because it addresses real problems. As you pointed out, one challenge is helping new users become more proficient faster, leveling the learning curve by guiding them on probe placement or labeling anatomy with AI assistance. The Kosmos product has been well-received, and we know you’re a fan. What stands out to you, especially considering your experience with various equipment?
José Mariz, MD: Kosmos excels in delivering high-quality 2D images. The engineering of the ultra-portable ultrasound machine and its probes is impressive. Another standout feature is its user-friendly interface, facilitating swift recording and sharing of images and videos with colleagues, setting it apart from other machines. The exceptional 2D image quality and user-friendly interface make Kosmos remarkable.
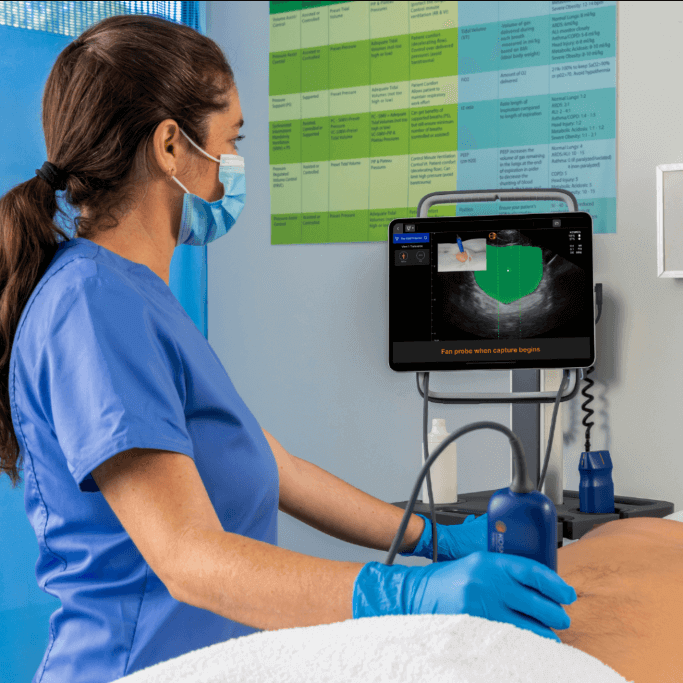
Artificial intelligence is the cherry on top, especially in teaching cardiological windows during immersive courses. It transforms the challenging task of teaching cardiological windows, making it akin to a gaming experience. Starting with a normal person as the baseline makes gaining confidence in identifying normal conditions easy. The machine-computer relationship shines, maintaining patience and guiding the user effectively.
Teaching complex cardiological exams can be daunting for students, who may feel they need more skills. Kosmos, with its artificial intelligence, proves invaluable in overcoming this challenge. My experience, along with evidence from a colleague’s detailed comparison with a control group of students, underscores three key strengths: a user-friendly application for immediate sharing, AI assistance in challenging cardiological teachings, and the overall excellence of the Kosmos system. I’m eager to explore its impact further, especially after learning about my colleague’s remarkable experiences in East Timor, a considerably impoverished region.
EchoNous: From your perspective, what’s on the horizon for point-of-care ultrasound? What does the future look like?
José Mariz, MD: In the future, I believe the stethoscope will become a thing of the past, much like bulky mobile phones evolved into today’s sleek devices. This transition marks the emergence of a new era—the fifth pillar of the physical exam. Just as it’s unimaginable to picture life without our modern phones, the same might soon be said about the ultra-portable ultrasound.
Firmly rooted in physics, ultrasound guarantees patient safety and stands out as the smartest imaging modality—even functioning in space. As our understanding of humanity expands, ultrasound will seamlessly become a part of medical education right from the first year. Artificial intelligence is a key player in this integration, which plays a crucial role in bridging gaps and elevating the intelligence and usability of machines.
We’re facing challenges in advancing probes and technology, aiming for a universal program for the physical exam. Looking ahead, students will streamline tasks efficiently using just one probe, optimizing their workflow. Ultrasound’s influence will stretch across professions, embraced by nurses and paramedics, seamlessly integrated into ambulances alongside oximeters and point-of-care blood analysis. This positions ultrasound as the fifth pillar in the physical exam, with technology playing a vital role in measuring blood pressure, oximetry, and ultrasound diagnostics.
EchoNous: Well said. Two studies explore the same thing—novice users achieving ejection fraction on par with expert users in real-world scenarios. Dr. Kumar led a study comparing AI and non-AI groups of novice users. Dr. Hibbert also released a study just a couple of weeks ago, exploring the same territory: novice users pulling off ejection fraction results on par with experts in the real world.
José Mariz, MD: Even seasoned physicians acknowledge the changes. Teaching ultrasound to my internal medicine fellows, with a focus on the heart’s function, was a complex task five years ago. What was once considered advanced and challenging has now become basic and easy, thanks to the guidance of the program.
Ultrasound’s evolution has been explosive, providing rapid insights into the heart’s function within minutes. The VExUS protocol, a concept from physiology, is now observable on machines, transforming treatment dynamics. While it may not drastically alter patient outcomes, it significantly improves efficiency and enhances doctors’ knowledge. Touching patients has been transformative for centuries, and now, with ultrasound, technology seamlessly aligns with humanity.
EchoNous: Thank you, Dr. Mariz, for your valuable insights into the evolving landscape of Point-of-Care Ultrasound. It’s been a pleasure discussing the transformative potential of POCUS and its role in shaping the future of medical practice. We appreciate your time and expertise. It’s very encouraging for us, and I’m sure it’ll be very encouraging for other folks.